
No Surgeon Operates Blind

No Surgeon Operates Blind, a point of view from Engage3P by Shera Haliczer
What Is the Client Actually Buying
Recently a new client asked me how I price my services. Fixed fee? Time and materials? The familiar ways change work has always been valued and billed.
I stopped him, because that runs against the entire reason I built Engage3P. Every one of those models prices the activity. The hours, the workshops, the deliverables, the production. And the production was never the thing a client actually needed.
I spent 25 years getting to that realization. The CHRO seat at top law firms, a decade leading HR technology strategy, and the global change programs underneath both, where transformation either lived or quietly died. From every one of those chairs I watched the same thing happen. A company commits real money to a transformation. The work gets done. The system goes live, the training gets delivered, the documents pile up. And then, often as not, nothing actually changes in how people work.
So the money moves and the activity happens, and the thing the client wanted, people working differently, does not arrive. For a long time I assumed the cause was execution, or budget, or the wrong vendor, or resistance. It was none of those. The cause sat further upstream, in a question nobody asked before the spending started: what is actually wrong here, and does anyone know before the work begins.
How a client pays for change has never been the problem. What they are paying for is. And the clearest way I have found to explain that has nothing to do with consulting.
No Patient Says Cut Me Open and See What You Find
When a person feels unwell, they go to a doctor, and the doctor does not reach for a scalpel. They run blood work. They order a scan, an MRI, a CT scan, X-rays. They find the problem before they consider an incision, because operating without a diagnosis is not treatment. It is gambling with a knife and the patient's life.
No patient has ever laid down and said, “cut me open from stem to stern, dig around, and if you find something wrong, fix it.” The idea is absurd. The cost is enormous, the risk is worse, and the odds of finding and fixing the real problem by rummaging are terrible.
That is the model traditional change management runs on. It starts cutting on day one. It stands up the workstreams, schedules the workshops, sends the communications, and begins asking questions, all while having no real idea what is actually wrong. The discovery is supposed to happen during the operation, if it happens at all. The organization is already open on the table before anyone has established what the procedure was meant to treat.
The results match the method. In Prosci's benchmarking, projects with poor change management meet their objectives only 13% of the time, against 88% for those that do it well [1]. A 2024 study across hundreds of projects found two thirds of companies running no formal change management at all [2]. The money churns, and most of it gets the organization nowhere, which is what a blind operation produces.

1 in 3 major change initiatives fully achieve their goals
Whatever that costs, and it costs a great deal, the spending was never the core problem. The core problem is that the cutting started blind.
No Patient Writes Their Own Chart
A doctor never hands the patient the clipboard and asks them for the diagnosis. The patient knows where it hurts. The patient does not know why. That is the doctor's job, and it is the part the patient came to pay for.
Consider a risk register. Anyone who has run a transformation has produced one. Look at what actually happens to make it. The people in the room are not junior staff filling in a form. They are the executives and the leaders, the most expensive minds in the building, and they spend their hours telling the consultant what they are worried about, while the client pays the consultant to sit there and write it down. The expert briefs the note-taker, and the meter runs the whole time.
And the brief is thin, because the people giving it only know what they were told. The exercise assumes they were told everything that is actually happening, which is rare, and sometimes they have barely been told anything at all. So the register captures fear, secondhand, from people working with partial information, and that fear becomes the plan.

Fear is not a diagnosis, an Engage3P principle on diagnosing before prescribing
The top line is the tell. The worst risk the team can name is that resistance is real and they cannot see where it lives. That is a patient saying it hurts somewhere and not knowing where. The response logged beside it is to run a stakeholder analysis to go and find it, which is the operation searching for the diagnosis it never had. Fear is not a diagnosis. A room can only name the dangers it can already picture, and the ones that sink a transformation are the ones nobody can picture yet.
The risk register, and the stakeholder analysis that traditional change management runs alongside it, are the instruments the field reaches for first. The problem is not that the work gets done poorly. It is that these instruments interrogate the project and never examine the people who have to live through it.
A Different Instrument Asks a Different Question
The fix is not a better risk register. It is a different set of instruments, pointed where the register never looks.
Engage3P does everything traditional change management does. It transforms the parts that never worked, and it adds the instruments nobody else has. Start with the one every transformation already leans on.
The risk register we do not transform. We replace it, because it was never built to answer the real question. It is a single lens, aimed at the project, and it never turns toward the people who have to carry the change.
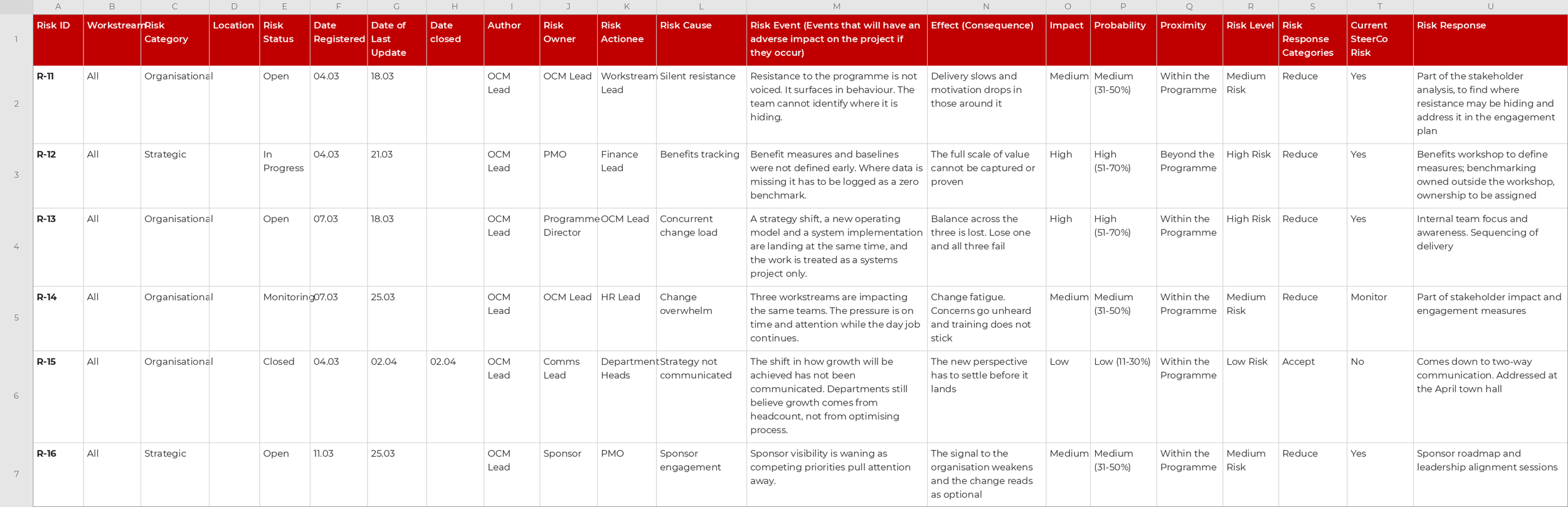
A traditional change-management risk register, a single project-focused lens that catalogues fear rather than diagnosing the cause
The risk register. One lens, aimed at the project, cataloguing fear.
In its place we build a diagnostic layer the register could never be, and the floor of it is MIA™. MIA™ studies the people who have to live the change, and whether they can absorb it at all right now. The old view examines the thing being installed. The new view examines the body it is being installed into. MIA™ assesses three capacities. Motivation, whether people see the purpose and have the energy to engage. Intention, whether they have clarity on what is expected. Attention, whether they have any room left to absorb something new. When any of the three drops, the symptoms are specific and predictable, and they are exactly the symptoms a team with no instrument writes down as risks.
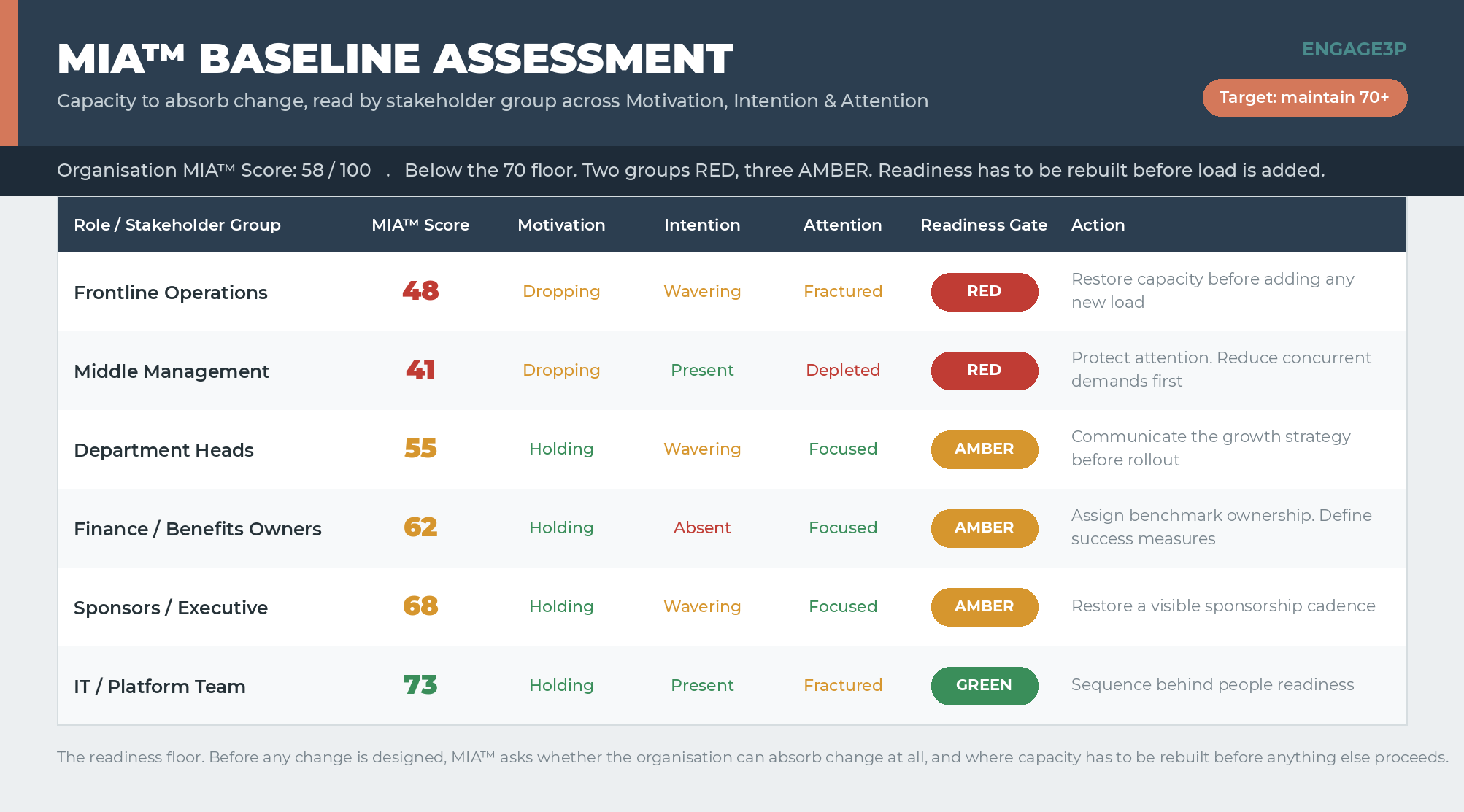
MIA Baseline assessment scoring stakeholder groups across Motivation, Intention and Attention, showing whether people can absorb the change at all
MIA™ Baseline. The readiness floor: whether the people can absorb the change at all.

When MIA drops, people go MIA, the Engage3P signature line on tracking human capacity through change
On that floor sits the Friction Map. It locates where the friction actually lives, across People, Process & Platform, and ties each source to the capacity it threatens. The Intervention Trigger Map sets the thresholds for action in advance, so the response to a problem is decided before the problem arrives, not improvised once the team is already behind. The register asked a room to name its fears. These read the organization and tell the truth.
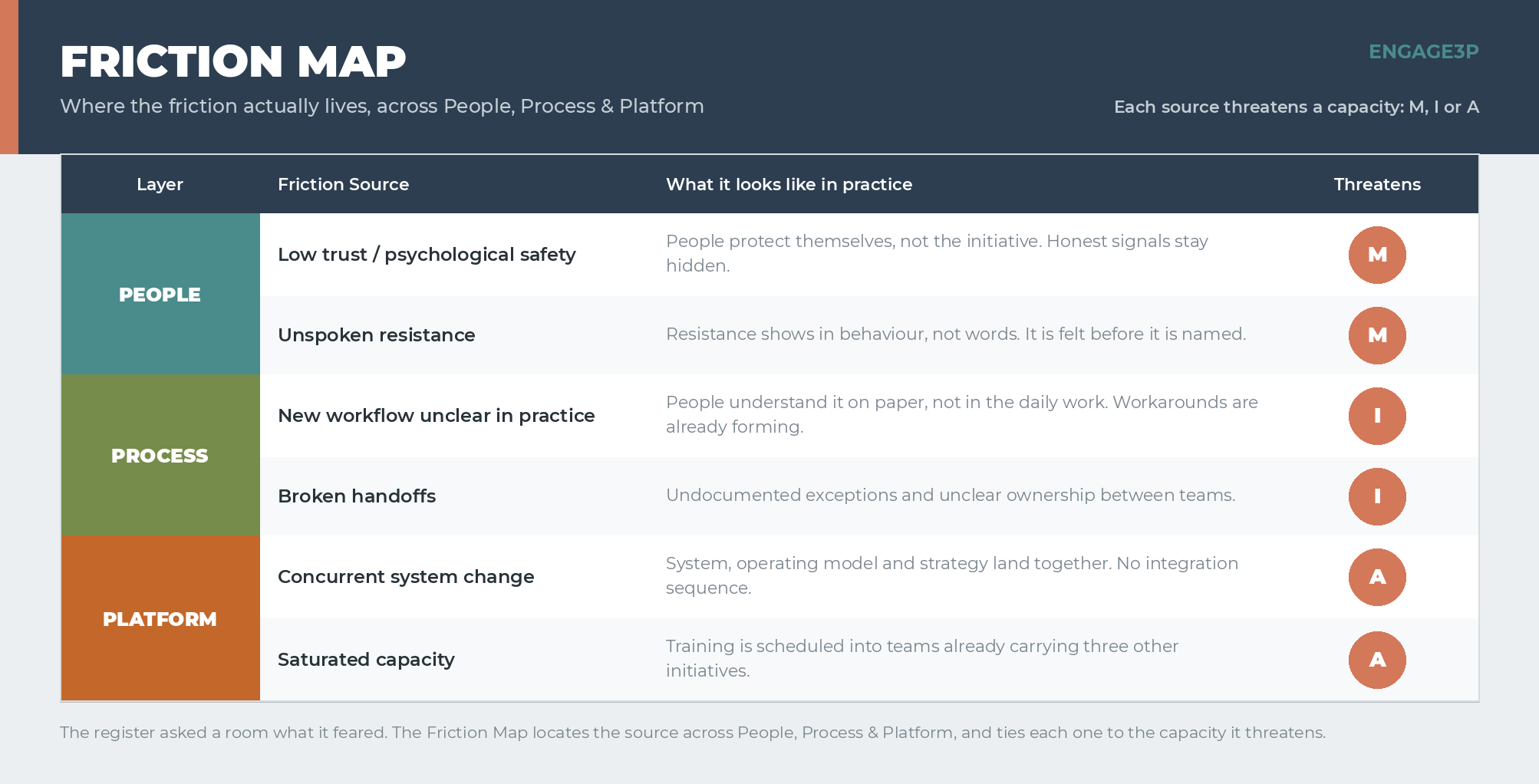
Engage3P Friction Map locating where friction lives across People, Process and Platform and tying each source to the capacity it threatens
Friction Map. Where the friction actually lives, across People, Process & Platform.
The register is not the only instrument we rebuild. Where traditional change management runs a stakeholder analysis, we build an Influence & Advocacy Map, a live read of who actually drives the change and who quietly stalls it, scored on capacity rather than seniority. Where it runs a change impact assessment, we build the Role-Based Success Clarity Map, which tells each person what success looks like for their role and, just as important, what to stop doing. The same jobs, finally given instruments that can do them.
The capacity problem is not a soft concern, and it is not a guess. The capacity to absorb change is collapsing, and it is measured. Gartner found that employees' willingness to support enterprise change fell to 43% in 2022, down from 74% in 2016, even as the average employee absorbed ten planned changes a year, up from two [3]. By 2024, in a Gartner survey of 473 HR leaders, 73% reported their people were fatigued by change and 74% said their own managers were not equipped to lead it [4]. The patient is already exhausted before the next operation gets scheduled. A risk register has no way to see that. MIA™ is built to read it first.
How One Pays for the Operation Does Not Change the Outcome
This is where the pricing question dissolves, the one I caught myself reaching for when speaking with this new client.
It does not matter whether the surgery is billed by the hour or quoted as a flat fee. Exploratory surgery is expensive, risky, and likely to miss the real problem regardless of how the invoice reads. A fixed fee feels safer because the number is fixed, but a fixed number on an undiagnosed problem is a confident guess, which is why the change orders always come. Hourly feels controllable until the meter runs through every workshop spent searching for the thing a diagnosis would have named in advance. Neither model is the disease. The disease is operating blind, and it drains the budget at any price.
The tools do not change it either. The production that once took a transformation weeks, the plans and decks and training, can be generated now in days. Faster production of the wrong treatment is still the wrong treatment, arriving sooner. Nothing automates the diagnosis that was never done.
What a client is buying, when the buying is done right, is not the operation and not the tools and not the hours. It is knowing what is wrong before the cutting starts.
Treatment That Heals, Not Treatment That Ends
A diagnosis is only worth having if what follows it heals. This is the second place traditional change management stops short, and it has its own surgical tell.
A change has two possible fates. Embodied means the patient is actually well, living differently because the body absorbed the change. Embedded means only that the incision is closed and healed. The system is live, the training is done, the process is documented, and on paper the operation looks complete. Traditional change management closes the incision and calls it a success. Adoption tracking asks whether people are using the new thing. Embodiment asks the only question that matters, whether the organization is genuinely healthier, working differently because the change took, not because a memo instructed it.
Think of the patient who comes through a flawless bypass, every artery cleared, and is back to the cheeseburger and fries inside the month. The procedure was perfect. Nothing about the life it was meant to save actually changed. The surgery was embedded. It was never embodied.

67 percent of workers experience burnout during change
I spent years in New York working near one of the great cancer hospitals in the world, and I would see patients out front in their gowns sitting in wheelchairs hooked up to an IV, brought outside to smoke. It has stayed with me, not as judgment, but as the hardest picture I know of how difficult real change is, even when the stakes could not be higher and the person knows it. A successful operation does not make a changed life. That is the gap, and it is exactly where transformations relapse. A flawless procedure, fully documented, that the body rejects the moment the surgeon leaves the room. Change that gets implemented but never lived is expensive theater, and a closed incision photographs just like a cure.
The people side is where the value actually sits. Prosci finds that excellent change management makes a project seven times likelier to meet its objectives [1]. Even that benchmark, though, measures whether the change was adopted, not whether it was embodied. That last distance, between used and lived, between closed and healed, is the one this firm exists to close.
How an Organization Diagnoses Before It Cuts
The alternative is not complicated, and it runs in the opposite order from the one on that register. Three moves. Diagnose the MIA™, Design for what the diagnosis found, Embody to last.
Diagnose first. Before a plan exists, read the organization's capacity across Motivation, Intention & Attention, and trace where the friction actually lives through the three places it ever comes from: People, Process & Platform, or the tension between them. The Friction Map does this work. Most firms operate on the platform or the process and never examine the people, which is why so many initiatives go live and then fade. The diagnosis names the real condition before money commits to treating the wrong one. Nothing can be honestly scoped or priced before this, which is the whole reason it comes first.
Design for what was found. With the condition identified, the treatment gets built for this organization's actual reality, not lifted from someone else's chart. It addresses the specific People, Process & Platform tensions the diagnosis surfaced, in the order they genuinely need addressing.
Embody to last. The work does not end when the system goes live, any more than recovery ends when the incision closes. It runs across six dimensions that continue past go-live: Diagnose, Design, Activate, Monitor, Adjust, Validate. Capacity gets read again during and after, because MIA™ moves as the change lands. And the engagement does not close on “it is installed.” It closes on Return on Intention™, the confirmation that the change was lived, delivered the value it was meant to, and left the organization stronger than it was found. That is the follow-up the unbenchmarked benefits on the register could never provide.
The depth is the client's to choose. Some need the diagnosis and a treatment plan and will carry it out themselves. That is Clarity and Strategy. Others want a partner who stays until the organization is genuinely well, not just sewn shut. That is Momentum. The depth is a choice. The diagnosis never is. Clarity is in every engagement, because prescribing without diagnosing is the entire error this piece exists to name.
None of it requires years or a permanent dependency. The diagnosis runs in weeks. The recommendations stay independent by design, with nothing to sell on the side. The goal is not a firm that never leaves. It is an organization that does not need one.
Run the Tests First
Every instinct in a transformation pushes toward cutting. Pick the system, stand up the teams, get moving, show progress. The register is what that instinct produces: motion in place of understanding, the patient's fears mistaken for a diagnosis, the operation underway before anyone knows what is wrong.
The better move is the one that feels slower and saves everything. Diagnose before you invest. Run the tests before the surgery. And the right moment for the tests is earlier than anyone schedules them, not the kickoff of the implementation, but the moment a leader first asks whether the change is even the right one, while the solution is still being chosen. The sooner the diagnosis runs, the more of the cost it can prevent.
The certainty a fixed fee seems to promise does not exist until the diagnosis does, and the cost of skipping it does not disappear. It arrives later, as the change that never landed and the budget that bought a closed incision instead of a cure.
That is where the work with Engage3P begins. Not with a scalpel and not with a year-long engagement. With a diagnosis of the MIA™, in weeks, that tells a leader what is actually wrong before the budget commits to fixing the wrong thing. From there, the depth is a choice.
Diagnose the MIA™. Design for Success. Embody to Last. How a client pays for change was never the question. Whether anyone diagnosed it before they started cutting always was.
Sources
[1] Prosci, The Correlation Between Change Management and Project Success (excellent change management makes a project roughly seven times likelier to meet objectives; 88% meet or exceed objectives with excellent change management against 13% with poor).
https://www.prosci.com/blog/the-correlation-between-change-management-and-project-success
[2] Işık (2024), study across 32 companies and 384 projects, via And Change (two thirds of companies report no formal use of change management).
https://www.andchange.com/why-project-success-demands-integrated-change-management/
[3] Gartner, via Harvard Business Review, Employees Are Losing Patience with Change Initiatives (willingness to support enterprise change fell to 43% in 2022 from 74% in 2016; the average employee faced ten planned changes a year, up from two).
https://hbr.org/2023/05/employees-are-losing-patience-with-change-initiatives
[4] Gartner newsroom, Leader and Manager Development Tops HR Leaders' List of 2025 Priorities (July 2024 survey of 473 HR leaders: 73% report employees fatigued from change, 74% say managers are not equipped to lead it).

Engage3P, independent by design, diagnose before you invest